Spine
The vertebral column, also called the backbone, extends from the skull to the pelvis. It accounts for two-fifths of total body weight and is made up of connective tissue and a series of bones, called vertebrae, which are superimposed in the form of a column, hence the term spine.
The vertebral column is made up of 24 vertebrae + sacrum + coccyx and forms, along with the head, sternum and ribs, the axial skeleton.
Size
In the adult, the spine has approximately:
Male: 72 - 75 cm
Woman: 61 - 65 cm
Joints of the Vertebral Column
All vertebrae from C2 to S1 articulate by means of:
– Joints of the vertebral bodies
– Joints of the Vertebral Arches
- Articulations between joint processes
- Articulation between laminae, spinous and transverse processes
Joints of the Vertebral Bodies
The vertebral bodies are united in a joint classified as secondary cartilaginous and 3 structures guarantee both this union and the static and dynamic stability between the vertebral elements. Are they:
- The Intervertebral Discs
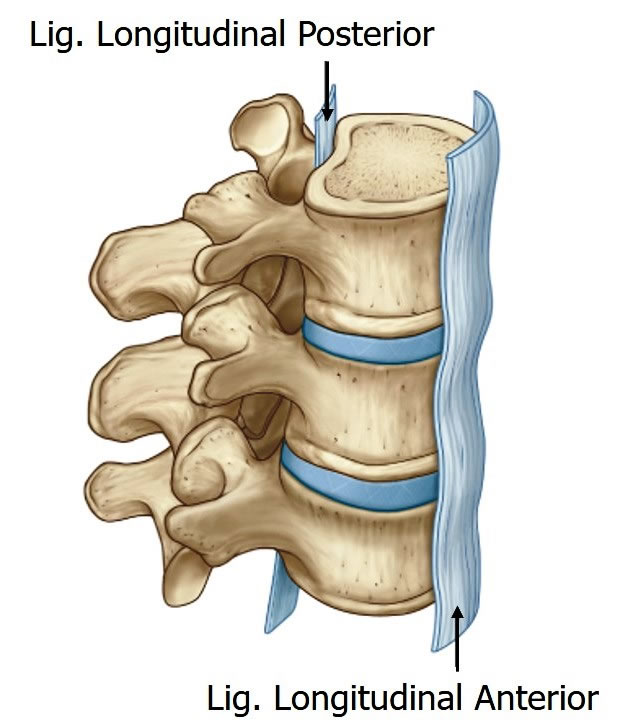
- The Anterior Longitudinal Ligament
- The Posterior Longitudinal Ligament
They are cartilaginous joints designed to support weight and resistance. Having as a relevant structure to be able to perform these functions the Intervertebral Disc.
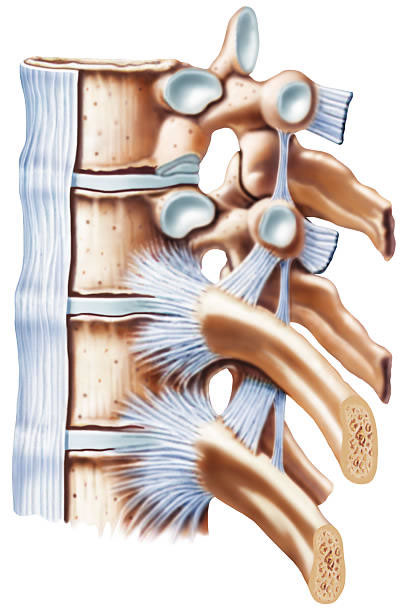
Intervertebral Disc
They are discoid-shaped skeletal elements made up of fibrous cartilage (fibrocartilage) that interpose between the vertebral bodies.
There are 23 intervertebral discs along the normal spine, which are located immediately below the body of the vertebrae, starting from the C2 vertebra (axis).
Thin terminal laminae separate the discs from their vertebral bodies.
End blades have important functions. The first is related to the nurturing function of the disc: they form a permeable barrier through which water and nutrients can pass between the nucleus pulposus and the cancellous bone of the vertebral bodies.
Secondarily, they have a mechanical role in preventing the bulging of the nucleus into the vertebral body.

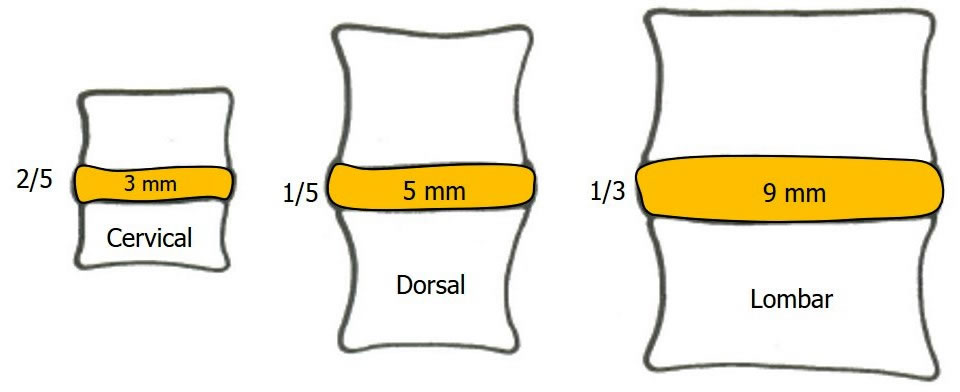
The sum of the height between the intervertebral discs corresponds to about 25% (20 to 33%) of the total length of the spine. They vary in shape, size and thickness in the course of the spine.
They are thickest anteriorly in the cervical and lumbar region and almost uniform in the thoracic region.
The discs are joined to the anterior and posterior longitudinal ligaments at the thoracic level, they are also joined laterally by intra-articular ligaments to the heads of the ribs that articulate with the adjacent vertebrae.
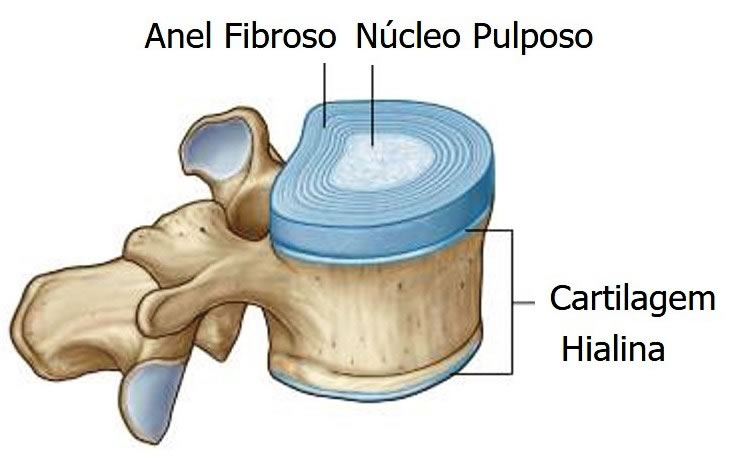
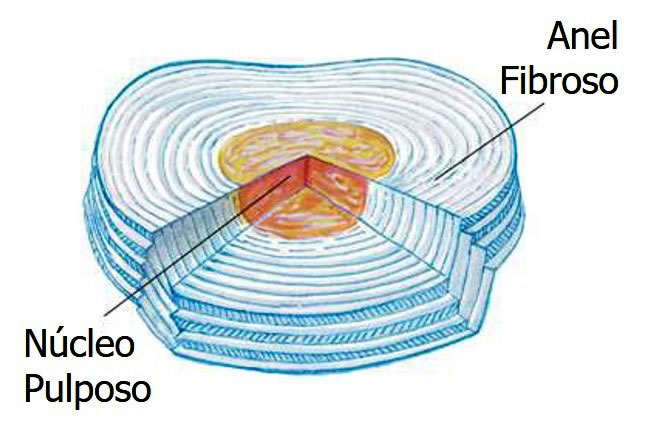
It consists of a peripheral fibrous disc composed of cartilaginous tissue ( FIBROUS RING ) and an internal, very elastic, soft, gelatinous substance ( PULPOSE NUCLEUS ).

FIBROUS RING
It consists of concentric lamellae of fibrocartilage, which form the circumference of the disc.
External part of the intervertebral disc consisting of fibrous cartilage with a predominance of collagen fibers.

The amount of collagen increases from the inner portion of the ring towards the outer.
The rings insert into the smooth, rounded epiphyseal rings situated on the articular surfaces of the vertebral bodies.
About 40% of the annular layers are incomplete in any part of the disc, however most of these are located in the posterolateral area.
In the lumbar spine, the anterior and lateral portions of the ring are approximately twice as thick as the posterior portion, making the posterior ring a weak area, thus being predisposed to trauma and degenerative changes.
PULPUS NUCLEUS
Central part of the intervertebral disc. It is more cartilaginous than fibrous and is normally very elastic.
It is a semi-fluid gel (40 to 60% of the total volume of the disc) consisting of fibrous cartilage with a predominance of proteoglycans in relation to collagen fibers, mainly type II.
Being a fluid, the core can be deformed under pressure without reducing its volume. This essential property enables it both to accommodate movement and to transmit some of the comprehensive load from one vertebra to another.

It acts as a shock absorber for axial forces and as a weight-bearing semi-liquid cushion during flexion, extension, and lateral rotation of the spine.
The nucleus pulposus is located more posteriorly than centrally and has a high H2O content that peaks at birth and decreases with advancing age.
The water content in the nucleus varies during life from 88% at birth to 65% in an individual aged 77 years (unlike what occurs in the annulus fibrosus, which maintains this content at about 70-75%).

Intervertebral Disc Functions
- dampen shocks
- absorb impacts
- alignment and union
- provide mobility
Compression on the intervertebral discs during flexion and extension movement of the spine.
Effects of vertical load on the spine
Vertical load is applied to the spine by the body's own weight, muscle action, ligament action, or an external load supported by the spine.
The result is a reduction in the height of the disc, with an increase in its diameter; deformation of cancellous bone and prolapse of the terminal laminae into the vertebral bodies.
In addition, there is the approximation of the ends of the articular processes that can be a factor of arthrosis, after some time.

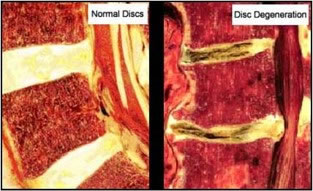
Healthy and injured discs respond differently to axial compression.
Intervertebral Disc Shape
The shape of the discs corresponds to that of the vertebral bodies and can be flat, domed and recessed. This fact is associated with the disc's resistance to bending and torsion.

Height of Intervertebral Discs
The height of the discs varies according to different regions of the spine and is related to the greater or lesser curvature and mobility of the vertebral regions.
The height of the discs can vary with:
- Age
- Congenital anomalies (sacralization and lumbarization)
- Pathology
- Diurnal variation (15-20 mm)
Vascularization of the Intervertebral Disc
For its nutrition, the disc depends on the diffusion of nutrients such as glucose, sulfate and oxygen. These reach the disk in two ways:
Annular : blood vessels on the periphery of the annulus fibrosus
Laminar : by capillary plexuses under the terminal laminae.
The laminar pathway of nutrition depends on the flow of fluid into and out of the disc, which in turn relates to posture and load on the spine.
The posterior edge of the disc has a poor nutritional supply.
The disc is avascular after age 10 (excluding the outer fibers).
Except for their periphery, which is supplied from blood vessels, the discs are avascular and supported by diffusion from the vertebral bones.

Anterior Longitudinal Ligament
It is a strong broad fibrous band that connects the anterolateral surfaces of the  vertebral bodies and discs.
vertebral bodies and discs.
It extends from the sacrum to the anterior tubercles of C1 and the occipital bone, anterior to the foramen magnum. It is continued superiorly with the anterior atlantoaxial ligament.
Wider caudally, but thick and narrow in the thoracic region and also narrower in front of the vertebral bodies than at the level of the intervertebral symphysis.
Occupation
It maintains the stability of the joints between the vertebral bodies and helps to prevent hyperextension of the spine.
| ANTERIOR LONGITUDINAL LIGAMENT |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Posterior Longitudinal Ligament
It is a much narrower band, slightly weaker than the anterior longitudinal ligament. 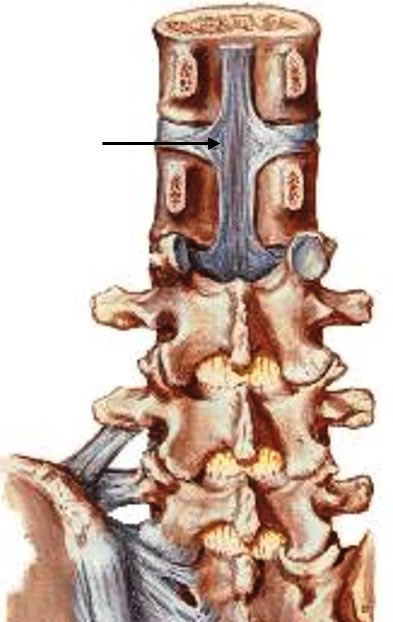
Runs within the vertebral canal along the posterior surface of the vertebral bodies. It attaches to the intervertebral discs and the posterior margins of the vertebral bodies from C2 to the sacrum. It continues superiorly with the tectorial membrane.
Occupation
Helps prevent hyperflexion of the lumbar spine and herniation and posterior protrusion of discs.
| POSTERIOR LONGITUDINAL LIGAMENT |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Joints of the Vertebral Arches
They are joints of the articular processes (zygoapophyseal).
Each joint is surrounded by a thin, loose joint capsule. The capsule is attached to the edges of the articular processes of adjacent vertebrae.
The joints of the articular processes allow for gliding movements between the vertebrae: the shape and arrangement of the articular facets determine the type of movement possible.
Accessory Joints
The joints of the articular processes allow for gliding movements between the vertebrae: the shape and arrangement of the articular facets determine the type of movement possible.

Yellow Ligament
It is a broad yellow elastic fibrous tissue that joins the laminae of the vertebral arches.
It holds the lamina above to the lamina below, thus holding the laminae of adjacent vertebrae together, forming the posterior wall of the vertebral canal. It has a certain elasticity that serves to preserve the vertical posture.
Yellow ligaments are long, thin and wide in the cervical region; thicker in the thoracic region and even more in the lumbar region.
Occupation
Prevent lamina separation, normally preventing injury to intervertebral discs
The strong elastic yellow ligaments help to preserve the normal curvatures of the spine and help to straighten the spine after flexion.
| YELLOW LIGAMENTS |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
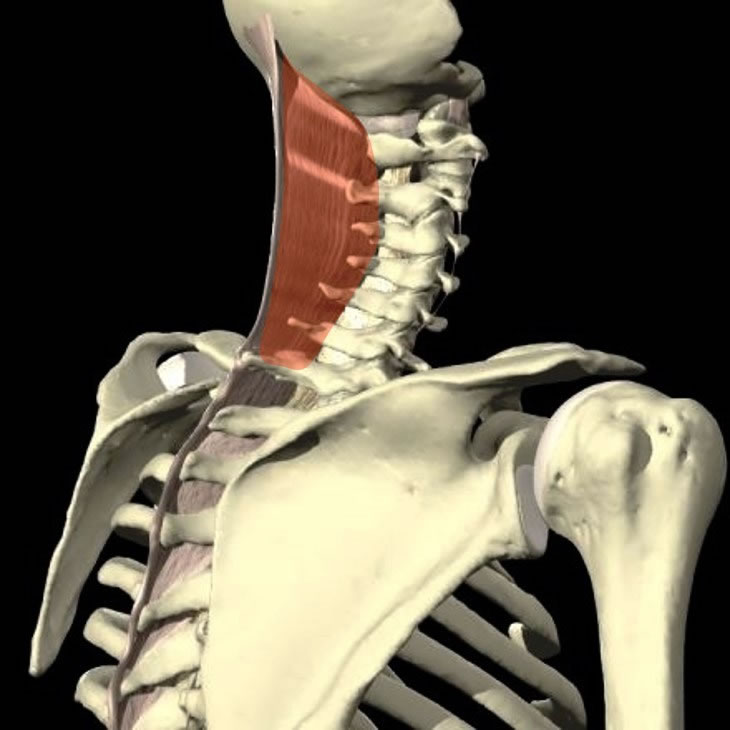
neck ligament
Intermuscular septum fibroelastic and often considered homologous with the supraspinous and interspinal ligaments of the neck.
It is composed of thick fibroelastic tissue that extends from the external occipital protuberance and posterior margin of the foramen magnum to the spinous processes of the cervical vertebrae.
| NUCHAL LIGAMENT |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
supraspinal ligament
Tough, fibrous ligament joining the apices of the spinous processes from the C7 to the sacrum (thicker and wider at the lumbar levels and intimately blended with the adjacent fascia.
Between C7 and the external occipital protuberance it is expanded like the nuchal ligament.

Interspinal Ligament
Thin and almost membranous, they unite adjacent spinous processes, their insertions extending from the root to the apex of each. They meet the ligaments flavum in the front and the supraspinatus ligaments in the back.

Occupation
They prevent the separation of the spinous processes, that is, the flexion movement of the spine.
| supraspinatus and interspinal ligaments |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Intertransversal Ligament
Between the adjacent transverse processes, they are made up of scattered fibers in the cervical region and fibrous cords in the thoracic region. The intertransverse ligaments of the lower back are thin and membranous.
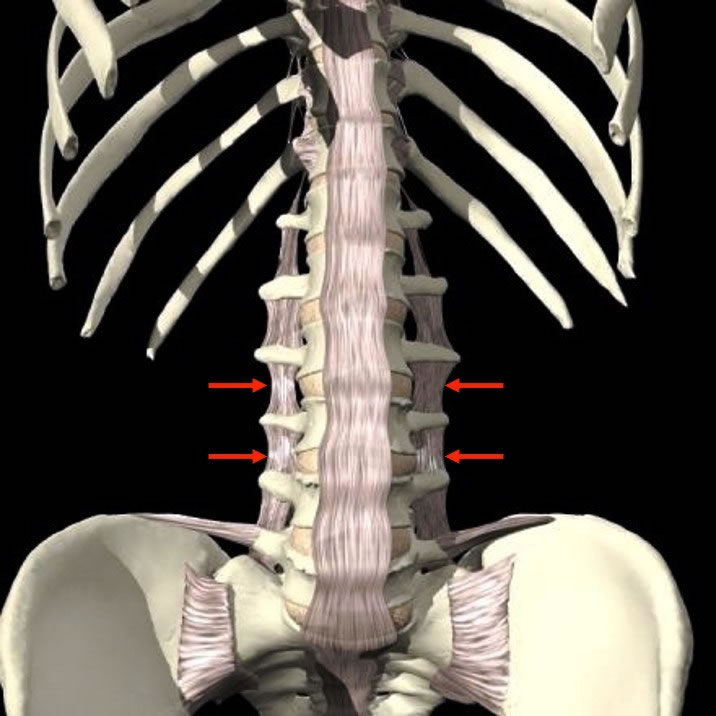
Occupation
They prevent the separation of the transverse processes, that is, the movement of lateral tilt.
| INTERTRANSVERSAL AND ANTERIOR LONGITUDINAL LIGAMENTS |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Atlanto-Occipital Joints (C0 – C1)
This joint is formed by the following structures:
Articular Capsules – surround the condyles of the occiput and articular facets of the lateral masses of the atlas.
Anterior Atlanto-Occipital Membrane – Wide and densely interwoven with fibers, it joins the anterior margin of the foramen magnum with the superior border of the anterior arch of the atlas.
Posterior Atlanto-Occipital Membrane – It is wide and thin and is attached to the posterior margin of the foramen magnum and the superior border of the posterior arch of the atlas.
Lateral Atlanto-occipital Ligaments – are thickened portions of the joint capsules reinforced by bundles of fibrous tissue and obliquely directed superiorly and medially. Insert into the jugular process of the occipital bone and the base of the transverse process of the atlas.
| ATLANTO-OCCIPITAL LIGAMENTS (C0 - C1) |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Occipito-Axial Ligaments (C0 – C2)
This joint is formed by the following structures:
Tectoric Membrane – is an extensive and resistant band that covers the tooth and its ligaments within the vertebral canal. It is considered the prolongation of the posterior longitudinal ligament. It is inserted in the body of the axis and superiorly in the basilar sulcus of the occiput.
Alar ligaments – start on either side of the apex of the tooth of the axis and insert into the rough medial part of the condyles of the occiput.
Apical Ligament of the Tooth – extends from the apex of the tooth on the axis to the posterior border of the foramen magnum, between the alar ligaments.
| OCCIPITO-AXIAL LIGAMENTS (C0 - C2) |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Atlanto-Axial Joints (C1 – C2)
The articulation of the atlas with the axis comprises the following structures:
Articular Capsules – are thin and loose and join the margins of the lateral masses of the atlas to those of the posterior articular surface of the axis.
Anterior Atlanto-Axial Ligament – is a strong membrane, attached to the inferior border of the posterior arch of the atlas and to the ventral surface of the axis body.
Posterior Atlanto-Axial Ligament – is a thin, broad membrane inserted into the lower edge of the posterior arch of the atlas and the upper edge of the axis blades.
Transverse Atlas Ligament – is a thick, strong, arched band that keeps the tooth in contact with the anterior arch. It inserts into the basilar part of the occiput and on the posterior surface of the body of the axis. The transverse ligament of the atlas together with the superior and inferior longitudinal fascicles form the cruciform ligament .
| UPPER CERVICAL REGION LIGAMENTS |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Costovertebral Joints
These joints are divided into two parts:
1 – Articulation of the head of the rib with the vertebral body;
2 – Costotransverse joint, where the neck of the rib articulates with the transverse process of the thoracic vertebrae.
1 – Rib Head Joint – is a flat joint formed by the articulation of the head of the rib with the vertebral body of the thoracic vertebrae. The ligaments of this joint are:
Articular Capsule – consists of short and resistant fibers joining the heads of the ribs to the joint cavities formed by the vertebrae and intervertebral discs.
Radiate Ligament of the Rib Head – joins the anterior parts of the heads of the ribs to the bodies of two vertebrae and their intervertebral discs. It consists of three flat fascicles that insert into the anterior part of the head of the ribs.
Rib Head Intra-articular Ligament – is a short, flattened bundle, inserted laterally into the crest between the articular facets and medially into the intervertebral disc, dividing the joint (each with its own synovial membrane).
| RADIATED LIGAMENT |
| |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
2 – Costotransverse Joint – is the joint between the articular facet of the tubercle of the rib and the transverse process of the corresponding vertebra. It consists of the following structures:
Joint Capsule – is thin and inserted into the joint circumference with a synovial lining.
Superior Costotransverse Ligament – attaches to the upper border of the neck of the rib and the transverse process of the vertebra above.
Posterior Costotransverse Ligament – These are fibers that attach to the neck of the rib and the base of the transverse process and lateral border of the articular process of the vertebra above.
Rib Neck Ligament – These are short, strong fibers that unite the back of the rib neck with the adjacent transverse process.
Rib Tubercle Ligament – is a short, thick, and strong fascicle that runs from the apex of the transverse process to the non-articular portion of the rib tubercle.
| COSTOTRANSVERSAL LIGAMENTS |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
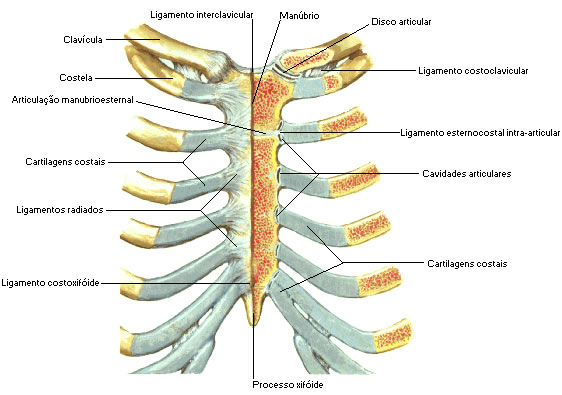
Sternocostal Joints – the joints of the cartilages of the true ribs with the sternum are flat joints, with the exception of the former which is a synchondrosis. The connecting elements are:
Joint Capsule – These are very fine fibers that surround the joints of the costal cartilages of the true ribs with the sternum.
Radiate Sternocostal Ligament – Thin, radiating bundles that radiate from the anterior and posterior surfaces of the sternal ends of the cartilages of the true ribs.
Intra-articular Sternocostal Ligament – constant only on the second rib. It extends from the cartilage of the rib to the fibrocartilage that joins the manubrium to the body of the sternum.
Costoxiphoid Ligament – attaches the anterior and posterior aspects of the seventh rib to them in the xiphoid process.
| STERNOCOSTAL JOINTS |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Interchondral Joints – joints between the costal cartilages.
Costochondral Joints – joints between the ribs and costal cartilages.
Sternal Joints :
1 – Manubrium-sternal – between the manubrium and the body of the sternum, it is usually a symphysis.
2 – Xiphosternal – between the xiphoid process and the body of the sternum, it is usually a symphysis.
Lumbosacral Joints
These are the joints between the 5th lumbar vertebra and the sacrum bone. Their bodies are joined by a symphysis, including an intervertebral disc.
Ileolumbar ligament – inserted into the anteroinferior surface of the 5th lumbar vertebra and radiates into the pelvis through two bundles: an inferior one, the lumbosacral ligament that inserts into the anterosuperior aspect of the sacrum and a superior bundle, the partial insertion of the muscle quadratus loin, passing to the iliac crest anterior to the sacroiliac joint, continuing above with the thoracolumbar fascia.
| ILEOLUMBAR LIGAMENT |
 |
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |
Sacrococcygeal joint
This is a symphysis between the apex of the sacrum and the base of the coccyx, joined by a fibrocartilaginous disc.
Anterior Sacrococcygeal Ligament – irregular fibers that descend over the pelvic surfaces of both the sacrum and the coccyx.
Posterior Sacrococcygeal Ligament – Superficial passes from the back of the fifth sacral vertebra to the back of the coccyx.
Lateral Sacrococcygeal Ligament – connects a transverse process of the coccyx to the inferolateral angle of the sacrum bone.
Intercorneal Ligaments – join the horns of the sacrum and coccyx.
| SACROCOCCYGEAL JOINT |

|
| Source: NETTER, Frank H.. Atlas of Human Anatomy. 2nd edition Porto Alegre: Artmed, 2000. |